Coronary Artery Bypass Surgery
Your coronary arteries are the vessels that carry blood to your heart muscle. If one or more of these arteries are blocked, blood can’t flow to the heart muscle. In this case, part of the heart muscle may die (heart attack). Or it may become weakened and damaged and cause chest pain (angina). You may have shortness of breath, increasing tiredness (fatigue), leg swelling, or a run-down feeling. Coronary artery bypass surgery makes a path for blood to flow around a blockage. It helps reduce the risk for more damage to your heart caused by the lack of blood. It may also ease your symptoms of angina or shortness of breath.
Getting ready for surgery
Prepare for the procedure as you have been instructed. In addition:
-
Tell your healthcare provider about all medicines you take. This includes over-the-counter medicines. It also includes herbs and other supplements and any recreational drugs. You may need to stop taking some or all of them before surgery. Your healthcare team will tell you which to take or stop. Pay attention to which medicines you need to take the day of surgery and which you should stop before surgery. Make sure you know when medicines should be stopped.
-
If you smoke, use smokeless tobacco, electronic cigarettes, or vaping devices, you should quit before your surgery.
-
Follow all directions you are given for not eating or drinking before surgery. Most people are told to not eat or drink anything after midnight before their procedure.
Being on a heart-lung machine
Coronary artery bypass surgery can be done with the heart still beating (off pump) or with the heart stopped (on pump). Your surgery team can tell you more about which type of surgery you will have:
-
On-pump surgery. A machine does the work of your heart and lungs during surgery. Blood is circulated through the heart-lung machine. The machine supplies the blood with oxygen and pumps it back through the body. In these cases, the heart may be stopped temporarily before the graft is attached. Your own heart and lungs start working again after the bypass is done.
-
Off-pump surgery. The heart-lung machine is not used, and the heart is not stopped. This is sometimes called a "beating heart" procedure.
There are risks and benefits of each method. If you have a question about why your doctor is using one method instead of the other, don't be afraid to ask.
Preparing the bypass graft
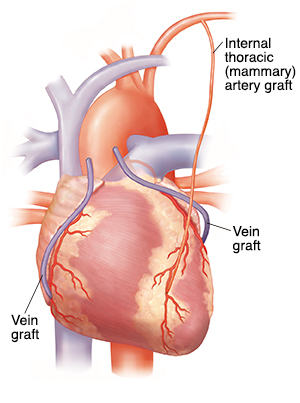
First, a healthy blood vessel (graft) is taken from another part of your body. Taking this graft usually doesn't affect blood flow in that body part. Often there is more than one blockage in the coronary artery. If you have more than one blockage, you may need more than one graft. You may have special ultrasound tests to look at the possible grafts before surgery. One or more of these blood vessels will be used for the graft:
-
The saphenous vein, which is in the leg
-
The radial artery, which is in the wrist
-
The internal thoracic (mammary) arteries, which are in the chest wall. There are two internal thoracic arteries, one on each side of the chest. Most often, the left artery is used, but sometimes both are used.
Reaching the heart
While one member of the bypass team is harvesting the graft or grafts, another member works to reach your heart. The provider makes an incision in your chest. Then they open the breastbone (sternum) down the middle and pull it apart. The breastbone is held open during surgery. This puts pressure on the nerves of the chest. This is why you may have soreness and muscle spasms in your chest, shoulders, and back after surgery.
Attaching the graft
A small opening is made in the coronary artery, past the blockage.
If a saphenous vein or radial artery is used , one end of the graft is sewn onto this opening. The other end is typically sewn onto the aorta. Neither the diseased artery nor the blockage is removed. If a stent is in place, it is not removed either. This is because the stent will already have become a permanent part of the artery.
If the internal thoracic (mammary) artery is used , one end of the graft is sewn onto this opening. The other end is already attached to a branch of the aorta.
Finishing up
Once the graft has been attached, blood will start flowing through this new pathway to bypass the blockage. If you have multiple blockages, more than one bypass may be done. Then your breastbone is rejoined with wires. These wires will stay in your chest permanently. They rarely cause a problem. They are safe around airport metal detectors and in MRI machines. The incision is closed, and you are taken to the intensive care unit (ICU) to begin your recovery.
Risks and possible complications
You and your surgeon can discuss the risks and possible complications of coronary artery bypass surgery. They may include:
-
A lot of bleeding that means you need a blood transfusion or more surgery
-
Infection of the incision sites
-
Lung infection (pneumonia) and other infections
-
Fast, slow, or irregular heartbeat (often temporary)
-
Slow heart rate that can mean you need a permanent pacemaker inserted
-
Nerve injury or muscle spasms
-
Breathing problems
-
Memory problems or confusion
-
Heart attack, stroke, or death
-
Damage to other parts or organs of your body